A consultation has a window. It opens when the patient sits down and begins to close the moment uncertainty takes hold. Most surgeons sense this: the shift in body language, the questions that start repeating, the pause before “I’ll think about it.” What is less understood is exactly when that window closes, and what keeps it open.
This is not a question of persuasion. Patients who leave without booking are not unconvinced by their surgeon. They are unconvinced by their own ability to imagine the outcome. That distinction matters, because the solution is not a better sales technique. It is a faster path to certainty.
The practices reporting the highest consultation conversion rates are not the ones with the most experienced surgeons or the lowest prices. They are the ones that remove uncertainty earliest in the appointment.
Supported by: Kurola et al., “Three-dimensional Simulation on Patient-reported Outcomes Following Oncoplastic and Reconstructive Surgery of the Breast,” PRS Global Open, May 2024.
Where consultations lose momentum
The structure of a typical aesthetic consultation follows a recognizable pattern. The surgeon reviews the patient’s concerns, discusses the procedure, explains the expected outcome, and answers questions. It is thorough. It is also almost entirely verbal.
The problem with verbal explanation is that it places the entire cognitive burden on the patient. They must take what the surgeon is describing, a result that does not yet exist, on a body they see differently than anyone else does and construct a mental image accurate enough to make a permanent decision about. Most cannot do it. Not because they lack intelligence, but because that is an extraordinarily difficult thing to ask of anyone.
This is where consultations stall. Not at the price discussion. Not at the risk explanation. At the moment the patient tries to picture the outcome and cannot hold the image with enough confidence to commit to it.
Uncertainty is not the same as doubt
There is an important distinction between a patient who doubts the surgeon and a patient who is uncertain about the outcome. Doubt is about trust. Uncertainty is about information. A patient can have complete confidence in their surgeon and still leave without booking because they cannot clearly see what they are agreeing to.
This distinction changes the approach. If the problem were doubt, the solution would be rapport, credentials, and testimonials. But if the problem is uncertainty and the evidence suggests it is then the solution is visual. Give the patient something concrete to look at, something built from their own anatomy, and the decision becomes substantially easier to make.
The question is how quickly that visual is available in the consultation, and how closely it reflects surgical reality.
What the data shows
Clinical data from Arbrea’s published studies shows a surgical conversion rate of approximately 87%. In formal trials, the implant selection projected by the simulation matched the final surgical decision 98% of the time. Independent clinical validation, published in the Aesthetic Surgery Journal Open Forum, further confirms the accuracy of Arbrea’s 3D simulation in consultation settings.
Those two numbers are connected. The 98% accuracy figure is not just a measure of planning precision it is the reason the conversion rate holds. When a patient sees a simulation that reflects what surgery will actually produce, their decision is grounded in reality. They are not saying yes to a best-case scenario. They are saying yes to a verified plan.
In virtual consultations, where the surgeon and patient are not in the same room Arbrea’s tools produced conversion rates comparable to in-person appointments. The visualization removed the disadvantage of distance.
Source: Arbrea Labs, “New Clinical Evidence Confirms: Arbrea Achieves 100% Surgical Accuracy and High Conversion Rates in Virtual Consultations,” Plastic & Reconstructive Surgery – Global Open, November 2025.
Arbrea’s AR, 3D & AI tools preview generates an outcome in under 90 seconds from the start of the process. That is within the opening minutes of a consultation before uncertainty has had time to compound, before the patient has started mentally rehearsing reasons to wait.
The cost of a consultation that ends without a booking
A consultation that does not convert is not a neutral outcome. It carries a direct cost that most practices do not calculate explicitly.
Surgeon time is the most visible figure. A 45-minute consultation that ends without a booking represents 45 minutes that could not be allocated to a procedure or a converting patient. Room time, administrative preparation, and any pre-consultation imaging or measurements add to that figure. Follow-up communication, emails, calls, additional questions often doubles the time investment before the patient either books elsewhere or stops responding.
The less visible cost is what the patient does after leaving. They continue researching. They find other clinics. They book a second consultation somewhere else, often with a practice that has a stronger visual tool, and they make their decision there. The first surgeon did the work of building trust and clinical confidence. A competitor captured the booking.
The consultation that ends with “I’ll think about it” rarely converts later. Data from multi-site clinical observations indicates that patients who leave without booking following a visualization-supported consultation are significantly more likely to return than those who leave following a verbal-only consultation.
Source: Arbrea Labs multi-site clinical observations, Full data available at arbrea-labs.com
What the first five minutes should accomplish
The opening of a consultation should do one thing above everything else: establish what the outcome will look like for this specific patient. Not what outcomes generally look like for this procedure. Not what results other patients have achieved. What this patient, with this anatomy, can expect from this surgeon.
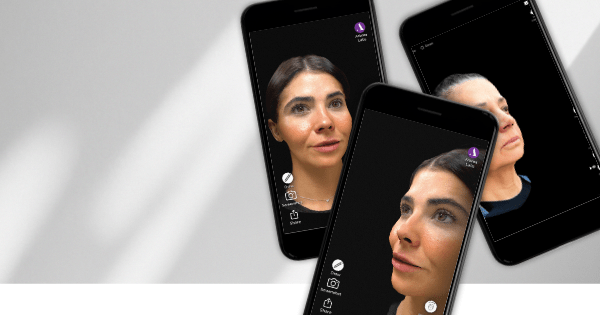
That requires a tool that operates from patient-specific parameters not edited photographs, not generic simulations, not drawings on a printed image. Arbrea’s AR, 3D & AI simulation builds from the patient’s own physical measurements. The AR preview places the projected outcome onto the patient’s body in real time, visible from multiple angles, on the iPad the surgeon is already holding.
When that happens in the first five minutes, the rest of the consultation changes. Questions become more specific. The conversation moves from “what will I look like” to “what size, what placement, what recovery.” Those are the questions of a patient who has already decided. The close is not a separate step, it follows naturally from a consultation where uncertainty was removed early enough that doubt never had room to form.
RELATED READING
”For me, 3D simulation is not just a visual tool, It’s a way to improve communication, align expectations, and help patients truly understand the potential outcomes of their procedure.
Dr. Carlos Cutini