For a surgical practice, patient education methods matter more than any single conversation. A good consultation isn’t one conversation. It’s a system.
Passive Patient Education Methods Don’t Move the Needle
The review’s clearest finding: a lecture transmits information efficiently, but it doesn’t change confidence, adherence, or outcomes much on its own. What moves those numbers is participation. Coaching, shared decision-making, peer support, family involvement, and simulation.
Simulation-Based Education Gets the Strongest Language in the Paper
Simulation-based education is credited with real skill mastery, higher patient confidence and self-efficacy, and fewer costly downstream events like readmissions. One cited trial found patients trained through simulation outperformed conventionally trained patients on an actual self-care skill, not just on a quiz afterward.
That’s a meaningfully different claim than “simulation is engaging.” It’s a claim that simulation, one of the most effective patient education methods the review covers, changes what patients can actually do.
Visualization and Shared Decision-Making
Shared decision-making shows up as its own category, separate from simulation. The review is specific about when it matters most: major, values-driven decisions with real tradeoffs, like choosing between surgical and non-surgical treatment.
The logic is simple. Patients can’t meaningfully weigh in on a decision they can’t picture. Decision aids close that gap by making options concrete enough to reason about. An AR simulation sits at the intersection of both categories. It’s simulation-based education and a decision aid at the same time.
Education Has to Continue After the Consultation Ends
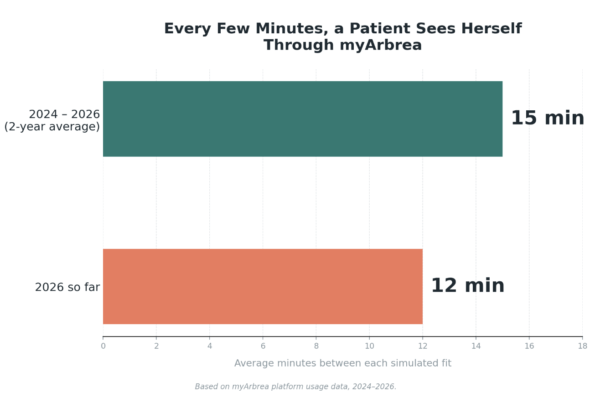
The review points to digital platforms, apps, and wearables as one of the few tools flexible enough to extend education past the office visit.
In a study of a digital prenatal platform, patients who used it more were significantly more likely to recognize warning signs and avoid unnecessary in-person visits. The relationship was dose-dependent. Continuous access isn’t a convenience feature. It’s the mechanism that turns one conversation into lasting comprehension.
20
82
5
Social Media Is a Real Channel, and a Real Risk
Platforms like Instagram, YouTube, and TikTok can reach people who’d otherwise never encounter reliable health information.
But the same channels spread misinformation just as fast. The review’s proposed fixes are broad: better health literacy, AI tools that flag bad information, closer platform collaboration, and a push toward verifiable sources. The review doesn’t name physician-led content as the fix directly, but the logic points there. A named, credentialed clinician is one of the clearest trust signals a patient has.
AI Is a Real Category Now, With Real Caveats
In a randomized trial cited in the review, an AI-enabled decision aid outperformed standard materials on decision quality, collaborative decision-making, and patient satisfaction, without adding consultation time.
The review also flags real limits: algorithmic bias, reading levels pitched too high for most patients, and a lack of clear sourcing. Its conclusion isn’t “deploy AI education tools.” It’s that AI should support the clinician, not replace them.
Why This Matters for Arbrea
AR simulation fits the review’s definition of simulation-based education, the category tied to changing what patients can do, not just what they understand.
Visualizing an outcome before treatment is the same mechanism the review names for improving shared decision-making. A patient-facing app extends education past the consultation, which the review treats as one of the harder problems in the field. Doctor-led content is a reasonable answer to the misinformation risk the review raises, even though the paper doesn’t name it directly. And AI used as a support layer under physician judgment is the same role the review describes for it.
Literaturverzeichnis
Lyu, X.; Li, J.; Li, S. Approaches to Reach Trustworthy Patient Education: A Narrative Review. Healthcare 2024, 12, 2322. https://doi.org/10.3390/healthcare12232322