Rhinoplasty has the highest revision rate of any aesthetic procedure. Estimates across published literature place secondary rhinoplasty rates between 5% and 15%, with some studies reporting figures higher in specific patient populations [1-2]. The clinical reasons are well documented: the nose heals unpredictably, oedema can persist for a year or more, and the structural complexity of the procedure leaves more variables in play than most other facial surgeries. But a significant share of rhinoplasty revisions are not driven by healing complications or technical outcomes. They are driven by a patient who expected something specific and received something different not because the surgeon underperformed, but because the preoperative consultation never established a shared, accurate visual reference for what the result would be.
That is a consultation problem. And it is one the rhinoplasty field has not solved, largely because the nose is the hardest result in aesthetic surgery to show before the procedure takes place.
The gap between what a rhinoplasty patient expects and what surgery produces is wider than in almost any other aesthetic procedure not because surgeons communicate poorly, but because the nose is three-dimensional, centrally positioned, and evaluated in relation to every other facial feature simultaneously. Verbal description of mm-level changes does not translate reliably into accurate patient expectation.
Why the nose is different
Every aesthetic procedure carries a communication challenge. The surgeon must convey an outcome that does not yet exist to a patient who cannot fully picture it. In most procedures, the transformation is significant enough that before-and-after references provide a reasonable approximation of the direction of change. The patient can look at comparable cases and form a broadly accurate expectation. Rhinoplasty does not work this way. The nose sits at the center of the face. Its appearance changes with every angle, every light source, every facial expression. A two mm reduction in dorsal height produces a result that looks dramatically different depending on the patient’s profile, their nasal tip projection, their facial proportions, and the relationship between their nose and their other features. The same surgical intervention produces a different visual result on every patient.
This means that reference images the tool most consultations rely on are almost useless for rhinoplasty. A patient who brings in a photograph of a nose they admire is not showing the surgeon what they want. They are showing them a nose that works on someone else’s face. Whether it will work on their face is a question that no reference image can answer.
What patients bring to rhinoplasty consultations
The typical rhinoplasty patient arrives with a collection of reference images assembled from social media, celebrity photographs, and filtered selfies. The quality of these references as surgical targets is consistently poor. Celebrity noses are photographed from specific angles under specific lighting conditions chosen to flatter. Social media images are frequently filtered or edited. Filtered selfies alter proportions in ways the patient may not consciously register. Beyond the quality of the references, there is a more fundamental problem. The patient is not requesting the nose in the photograph. They are requesting what they imagine that their nose would look like on their own face, a translation they perform mentally, without any reliable tools for doing so accurately. That translation is almost always wrong. The nose that looks balanced and refined on one face can look disproportionate or incongruous on another, and the patient has no way of knowing this until after surgery.
This is the expectation gap that drives rhinoplasty revisions. The surgeon delivered what was discussed. The patient received something different from what they imagined. Both statements can be simultaneously true, and in rhinoplasty they frequently are.
What Arbrea Face changes in the consultation
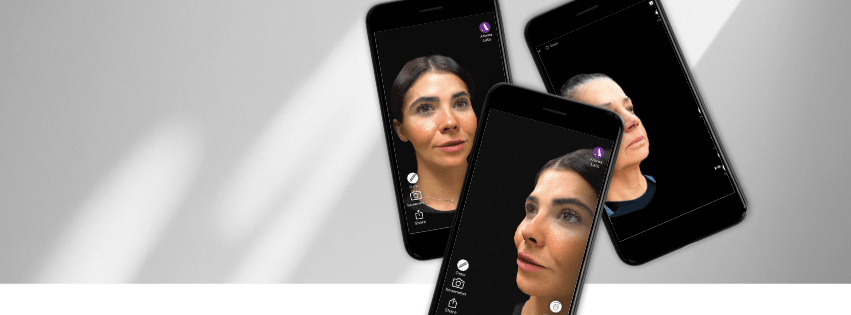
Cara Arbrea generates a patient-specific facial simulation from photographs taken during the consultation. The simulation is built from the patient’s own facial geometry, their proportions, their existing nasal structure, their facial relationships. When the surgeon adjusts nasal parameters in the simulation, the change is shown on the patient’s actual face, not on a generic model or a composite image.
For rhinoplasty consultations, this changes the nature of the conversation entirely. The patient is no longer being asked to imagine what a described change will look like. They are looking at it. The surgeon can show the effect of dorsal reduction, tip refinement, or alar modification on this patient’s face, from multiple angles, in the consultation room. The patient’s reference point shifts from a photograph of someone else’s nose to a simulation of their own outcome.
The rhinoplasty patient who has seen a patient-specific simulation of their outcome during the consultation is not asking the surgeon to match a photograph of someone else. They are asking for what they have already seen on their own face. That is a fundamentally different surgical target and a fundamentally lower risk of postoperative expectation mismatch.
The filler consultation where visualization matters just as much
Non-surgical rhinoplasty with dermal fillers presents a version of the same problem. The changes achievable with filler are smaller in magnitude than surgical rhinoplasty but no less difficult to communicate verbally. A patient who requests dorsal smoothing or tip definition with filler has the same difficulty picturing mm (inches) level changes on their own face as a surgical patient does.
Cara Arbrea applies equally here. A surgeon who can show a patient the projected result of a filler treatment on their own face before the treatment begins is having a different consultation from one who describes the expected change verbally. The patient understands what they are agreeing to. The surgeon understands what the patient expects. The margin for disappointment narrows significantly. There is also a conversion dimension. A patient who comes in for a filler consultation and sees, via Cara Arbrea, the limits of what non-surgical treatment can achieve for their specific anatomy is better placed to make an informed decision about whether surgical rhinoplasty is the more appropriate path. That conversation showing rather than telling a patient where filler stops being enough is one of the most clinically valuable uses of facial simulation in an aesthetic practice.
The At-Home Dimension: Where Lindapp Changes the Equation
There is a second consultation that rhinoplasty surgeons often overlook: the one the patient has with themselves, at home, after they leave the clinic.
Most patients considering rhinoplasty do not decide in the consultation room. They go home, look in the mirror, and spend days or weeks processing their decision. The mental image they work with during that time is often nothing more than a photograph from the consultation, and that photograph may already be lying to them. Perspective foreshortening, caused by inconsistent camera distance, angle, or settings, quietly distorts facial proportions in ways patients cannot detect. Unlike 2D filters or single-image simulations that compound this distortion, Arbrea’s technology corrects it by combining multiple images to cancel out angle-induced inaccuracies producing a simulation built on the patient’s true facial geometry, viewable in 3D from multiple angles and under different lighting conditions. This is a fundamental leap beyond what any 2D filter can offer.
Aquí es donde Lindapp extends the consultation beyond the clinic walls. Accessed privately from the patient’s own phone, it lets patients explore their 3D simulation at home, rotate it, examine it from the angles that matter to them personally, and share it with loved ones all without data stored in the cloud. Lindapp is intentionally designed as a lighter, more accessible companion to the full clinical platform the surgeon uses; it empowers the patient to arrive better prepared, not to replace the surgeon’s expertise. The goal is not for patients to make decisions alone at home, but to come to the next consultation having already processed the likely outcome more informed, less anxious, and ready for a deeper conversation.
When they are ready, they share their 3D scan directly with the surgeon. That moment of sharing is clinically valuable: the doctor receives richer facial data ahead of the consultation, and the patient arrives not as an uncertain lead, but as someone who has already visualized saying yes.
REFERENCES
[1] Broun F, et al. “Functional and Aesthetic Factors Associated with Revision of Rhinoplasty.” PRS Global Open, 2018. https://pmc.ncbi.nlm.nih.gov/articles/PMC6191217/
[2] “Revision Rhinoplasty: Incidence and Contributing Factors.” PRS Global Open, 2022. https://pmc.ncbi.nlm.nih.gov/articles/PMC9442826/